Compact vs Trabecular Bone: Key Differences Explained
Have you ever wondered what makes our bones both lightweight yet incredibly strong? The answer lies in the fascinating structure and composition of our skeletal system. Compact bone and trabecular bone are the two main types of bone tissue that give our skeleton its remarkable properties. While these tissues work together to support our body, they have distinct characteristics that serve unique purposes in our skeletal framework.
I've always been fascinated by how our bones manage to be both incredibly strong yet not too heavy. It's like nature's perfect engineering solution! In this article, we'll explore the differences between these two bone types and understand why this dual structure is essential for our daily movements and overall health.
Understanding Bone Tissue Types
Our skeletal system is a marvel of biological engineering. Bones provide structural support, protect vital organs, enable movement, store minerals, and even produce blood cells. To accomplish these varied functions, the body has developed specialized bone tissues. The two primary types are compact (cortical) bone and trabecular (cancellous) bone.
These bone tissues differ significantly in their structure, composition, and function. Their complementary properties allow our skeleton to be both strong and lightweight while serving various physiological needs. Understanding these differences isn't just academic—it helps explain how bone-related conditions develop and how we can better maintain bone health throughout our lives.
I remember learning about bones in my anatomy class and being surprised by how dynamic they actually are. Far from being static structures, bones constantly remodel themselves in response to stress, injury, and metabolic needs. Both compact and trabecular bone tissues participate in this ongoing renovation project, though at different rates and in different ways.
What is Compact Bone?
Compact bone, also known as cortical bone, forms the hard outer shell of all bones in our body. True to its name, it has a dense, tightly packed structure that makes it extremely strong and resistant to bending and torsion. This type of bone tissue makes up approximately 80% of the total bone mass in an adult human skeleton.
The basic functional unit of compact bone is the osteon (or Haversian system). Each osteon consists of concentric layers of bone matrix called lamellae, which surround a central canal (Haversian canal) containing blood vessels and nerves. These vessels deliver nutrients to bone cells (osteocytes) that reside in small cavities called lacunae. Tiny channels called canaliculi connect the lacunae, allowing osteocytes to communicate with each other and receive nourishment.
This highly organized structure gives compact bone its exceptional strength. In fact, compact bone can withstand weights of up to 5000 pounds! It primarily serves a mechanical and protective function, forming the shaft of long bones like the femur and humerus. Additionally, compact bone contains yellow bone marrow, which is rich in fat cells and serves as an energy reserve.
I've always thought it's incredible how something that appears so solid actually has this intricate microscopic plumbing system running through it. When you look at a cross-section of compact bone under a microscope, the osteons look a bit like tree rings—a beautiful example of how form follows function in nature.
What is Trabecular Bone?
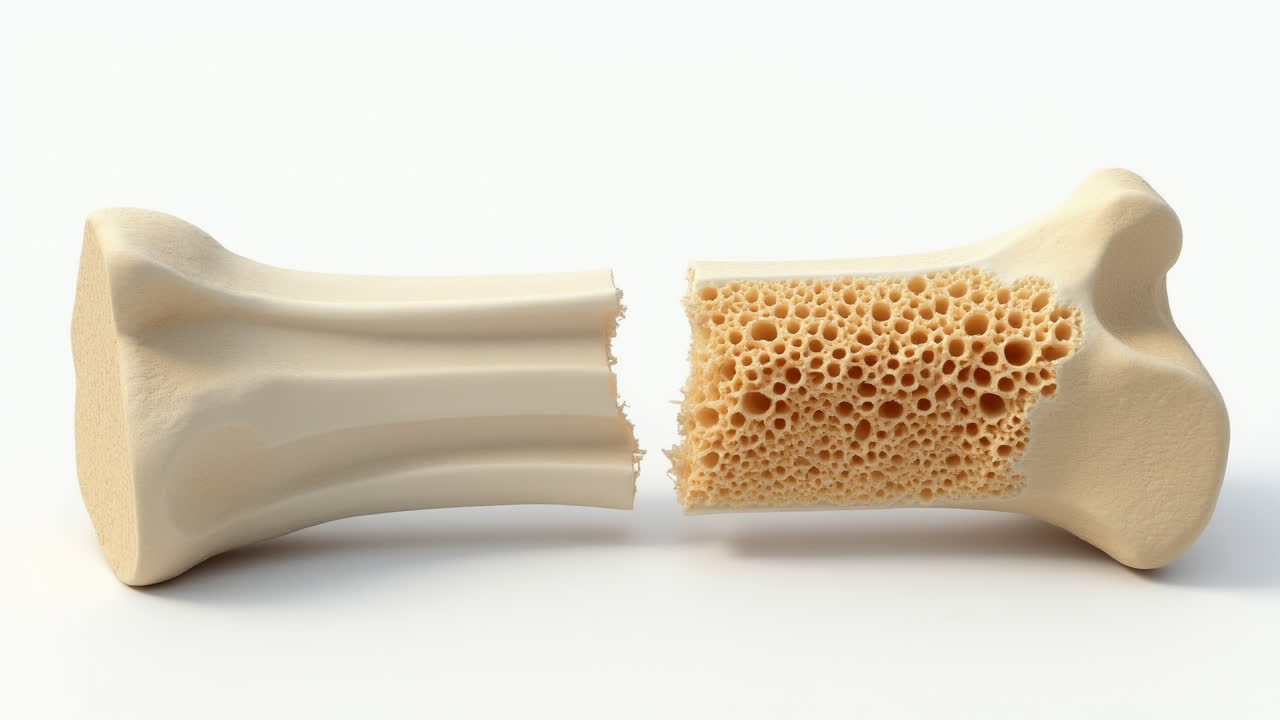
Trabecular bone, also called cancellous or spongy bone, has a strikingly different appearance and structure compared to compact bone. As its nickname suggests, trabecular bone resembles a sponge with its honeycomb-like network of connected plates and rods called trabeculae. These trabeculae create numerous small spaces, making this type of bone tissue much more porous than compact bone.
This specialized structure gives trabecular bone unique properties. While it's lighter and less dense than compact bone, the interconnected framework of trabeculae provides remarkable strength along lines of mechanical stress. Think of it as nature's version of an architectural truss system—distributing weight and absorbing shock efficiently.
Trabecular bone is primarily found in the ends of long bones, the interior of vertebrae, and in flat and irregular bones like the pelvis, ribs, and skull. The spaces between trabeculae are filled with red bone marrow, which is responsible for producing blood cells through a process called hematopoiesis. This explains why trabecular bone has higher metabolic activity compared to compact bone.
From a functional perspective, trabecular bone acts as a buffer for compact bone, absorbing and distributing forces throughout the skeleton. It's remarkably adaptive, with trabeculae continuously remodeling themselves in response to mechanical forces. This is why weight-bearing exercise strengthens our bones—the trabecular bone responds to this stress by building more connections!
I've often found it helpful to visualize trabecular bone as the internal scaffolding of a building, providing essential support while maintaining overall lightness. Without this ingenious design, our bones would either be too heavy for efficient movement or too weak to support our daily activities.
Comparison: Compact vs Trabecular Bone
While both compact and trabecular bone are essential components of our skeletal system, they differ significantly in many aspects. Let's examine these differences in detail to better understand how these two bone tissues complement each other in function and structure.
| Feature | Compact Bone | Trabecular Bone |
|---|---|---|
| Alternative Names | Cortical bone | Cancellous bone, Spongy bone |
| Location | Outer covering of bones | Inner cavity of bones |
| Structure | Dense, tightly packed osteons | Loose network of trabeculae |
| Porosity | Low (5-10%) | High (50-90%) |
| Functional Unit | Osteon (Haversian system) | Trabecula |
| Bone Marrow Type | Yellow bone marrow (fat storage) | Red bone marrow (blood cell production) |
| Weight Contribution | 80% of skeletal weight | 20% of skeletal weight |
| Primary Function | Structural support and protection | Shock absorption and hematopoiesis |
| Strength | Can withstand up to 5000 pounds | Less weight-bearing capacity |
| Calcium Content | High | Low |
This comparison illustrates how these two bone types have evolved to serve complementary functions in our skeletal system. Compact bone provides the strength and rigidity necessary for structural support and protection, while trabecular bone offers lightweight flexibility and houses vital metabolic functions.
I find it fascinating how our bones achieve such a perfect balance between these different tissue types. In areas that need maximum strength, like the shaft of the femur, compact bone predominates. In contrast, areas that need more flexibility and metabolic activity, like vertebrae, have a higher proportion of trabecular bone.
Similarities Between Compact and Trabecular Bone
Despite their structural and functional differences, compact and trabecular bone share several important similarities. Both are fundamental components of the skeletal system and play crucial roles in maintaining our body's overall health and function.
- Both contain the same basic cellular components: osteoblasts (bone-building cells), osteocytes (mature bone cells), and osteoclasts (bone-resorbing cells)
- Both are composed of bone matrix, which consists of organic components (primarily type I collagen) and inorganic mineral salts (calcium phosphate in the form of hydroxyapatite crystals)
- Both types undergo continuous remodeling throughout life in response to mechanical stress, hormonal signals, and metabolic needs
- Both provide attachment sites for muscles, tendons, and ligaments
- Both contain blood vessels and nerves, though in different arrangements
- Both contribute to mineral homeostasis, storing and releasing calcium and phosphorus as needed
These similarities highlight the unified nature of bone tissue despite its specialization into different types. It's a bit like how different rooms in a house serve different functions but still share fundamental attributes like walls, floors, and a connection to the overall structure.
I've always appreciated how our body develops specialized tissues that retain their fundamental characteristics while adapting to specific functional requirements. It's an elegant example of biological efficiency—using variations on a theme rather than creating entirely different structures.
Clinical Significance: Bone Disorders and Health
Understanding the differences between compact and trabecular bone has significant implications for bone health and disease. Various bone disorders affect these tissue types differently, and treatment approaches often need to consider these distinctions.
Osteoporosis, one of the most common bone disorders, primarily affects trabecular bone in its early stages. This makes sense when you think about it—trabecular bone has a higher metabolic activity and turnover rate, making it more susceptible to imbalances in bone remodeling. As osteoporosis progresses, compact bone is also affected, leading to increased risk of fractures.
Similarly, osteopenia, a condition characterized by lower than normal bone density (but not as severe as osteoporosis), tends to affect trabecular bone first. This is why bone density scans often focus on areas rich in trabecular bone, such as the spine and hip.
Other conditions like Paget's disease, osteogenesis imperfecta, and certain cancers can affect both bone types but may show preferential involvement of one type over the other. For instance, some bone tumors prefer to grow in trabecular bone due to its rich blood supply and metabolic activity.
From a therapeutic perspective, medications for bone disorders often target specific cellular processes in either compact or trabecular bone. For example, bisphosphonates, commonly used to treat osteoporosis, work by inhibiting osteoclast activity, which has a more pronounced effect on trabecular bone initially.
I remember talking with my aunt after she was diagnosed with osteoporosis. Her doctor explained that the condition had affected the trabecular bone in her spine and hips first, which is why those areas showed the most significant decrease in bone density on her DEXA scan. This real-world example helped me understand the clinical relevance of these bone tissue differences.
Frequently Asked Questions About Compact and Trabecular Bone
How do compact and trabecular bone respond differently to exercise?
Compact and trabecular bone respond differently to exercise due to their structural and metabolic differences. Trabecular bone, with its higher metabolic rate and greater blood supply, typically responds more quickly to weight-bearing exercises and resistance training. This is why exercises like walking, jogging, and weightlifting can improve bone density in the spine and hips (areas rich in trabecular bone) relatively quickly.
Compact bone also responds positively to exercise but generally takes longer to show significant changes. The mechanical loading from exercise stimulates osteoblast activity in both bone types, leading to increased bone formation. However, the response pattern follows what's known as Wolff's Law—bone adapts to the loads under which it is placed. This means that bone tissue develops along lines of mechanical stress, which can be particularly evident in the trabecular bone's architecture.
Do compact and trabecular bone age differently?
Yes, compact and trabecular bone demonstrate different aging patterns. Trabecular bone typically shows age-related changes earlier due to its higher turnover rate. After age 30-35, humans naturally begin to lose bone mass, with women experiencing accelerated loss after menopause due to declining estrogen levels.
In trabecular bone, aging leads to thinning and sometimes complete loss of trabeculae, resulting in a less connected network. This reduces the bone's ability to absorb and distribute forces, increasing fracture risk. In compact bone, aging causes an increase in porosity and a decrease in mineral density. Haversian canals may enlarge, and there might be reduced formation of new osteons.
These different aging patterns explain why vertebral compression fractures (involving primarily trabecular bone) are often among the earliest manifestations of age-related bone loss, while fractures of the femoral shaft (primarily compact bone) typically occur at more advanced stages of osteoporosis.
How do medications for bone disorders affect compact versus trabecular bone?
Medications for bone disorders often affect compact and trabecular bone differently due to variations in blood supply, metabolic activity, and cellular composition. Bisphosphonates (like alendronate and zoledronic acid), the most commonly prescribed medications for osteoporosis, initially show more significant effects on trabecular bone because of its higher remodeling rate and greater vascularity, which allows better drug delivery.
Anabolic agents like teriparatide (a parathyroid hormone analog) stimulate new bone formation and tend to have pronounced effects on trabecular bone first, improving its microarchitecture and connectivity. In contrast, denosumab, a RANK ligand inhibitor, shows robust effects on both bone types by powerfully suppressing bone resorption throughout the skeleton.
Hormone replacement therapy primarily affects trabecular bone in the early stages of treatment, which explains why it can quickly reduce the risk of vertebral fractures. Selective estrogen receptor modulators (SERMs) like raloxifene also show preferential effects on trabecular bone. Understanding these differential effects helps clinicians choose the most appropriate medication based on a patient's specific bone loss pattern and fracture risk profile.
Conclusion
The remarkable distinction between compact and trabecular bone represents one of nature's most elegant engineering solutions. By utilizing these two specialized bone tissue types, our skeletal system achieves an optimal balance between strength, weight, and metabolic function. Compact bone provides the durability and protection we need for daily activities, while trabecular bone offers flexibility, lightweight support, and houses vital blood-forming tissues.
This dual design allows our bones to adapt to various mechanical demands while serving multiple physiological functions. Understanding these differences isn't merely academic—it has profound implications for how we approach bone health, diagnose and treat bone disorders, and develop strategies for maintaining skeletal integrity throughout life.
As medical science advances, we continue to gain deeper insights into the complex relationship between these bone tissues and how they respond to aging, exercise, nutrition, and pharmacological interventions. This knowledge is crucial for developing more effective approaches to common bone disorders like osteoporosis and understanding how to optimize bone health through every stage of life.
Whether you're a healthcare professional, student, or simply someone interested in how your body works, appreciating the distinct yet complementary nature of compact and trabecular bone provides a fascinating window into the intricate design of our skeletal system. After all, it's this remarkable dual structure that allows us to move through the world with both strength and grace.